
Spinal Conditions: Neck Pain and Whiplash
Introduction
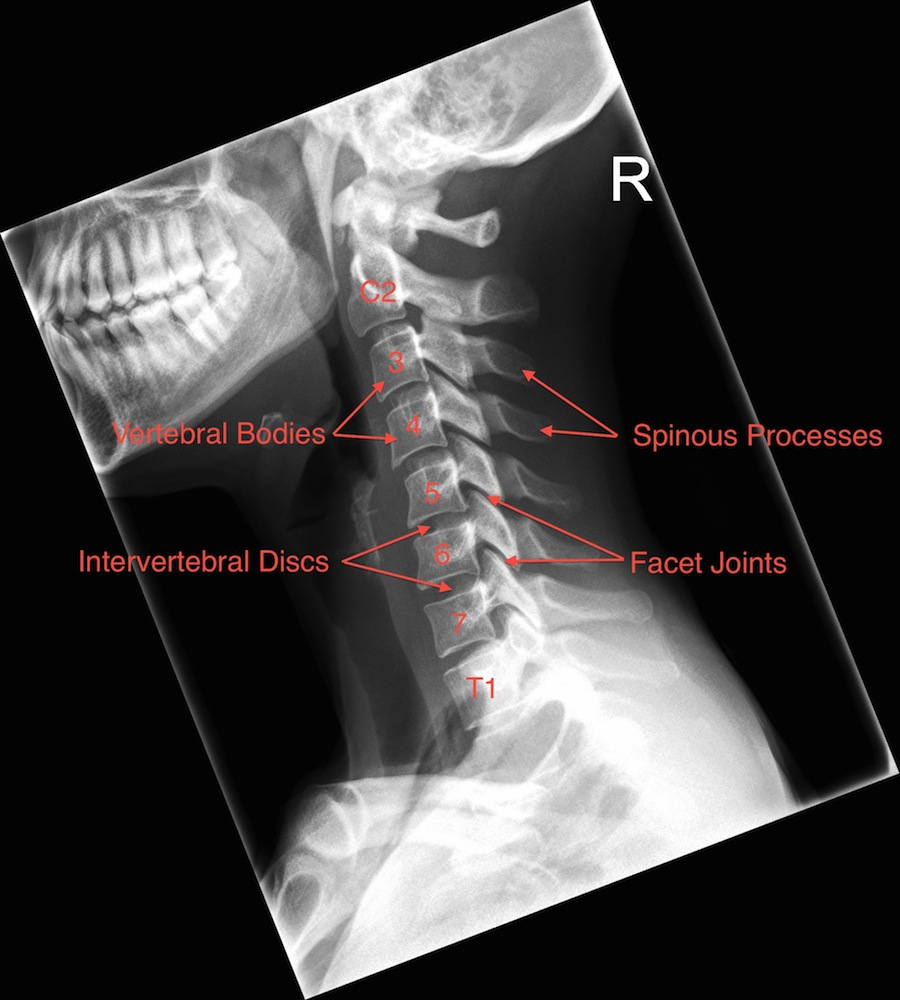
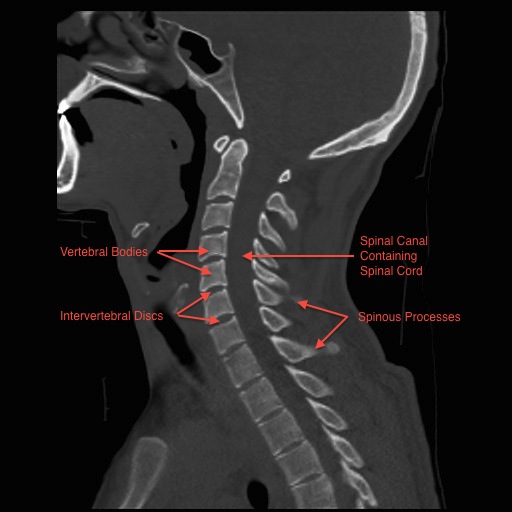
The neck (cervical spine) is composed of seven vertebrae that begin at the base of the skull and end at the upper back (see Anatomy Section). The upper two vertebrae are called the atlas and axis and they are different to the others. Over half of the movement of the neck occurs between the base of the skull and the axis. The neck has a significant amount of motion and supports the weight of the head. However, because it is less protected and more mobile than the rest of the spine, the neck can be vulnerable to motion related disorders producing pain and restricted motion. For most people, neck pain is a temporary condition that disappears with time.






Causes of Neck Pain
As with low back pain, it can be difficult to identify the exact source of neck pain. Red flags help healthcare professionals to determine whether something serious may be occurring. Neck pain can arise from the spine and from other non-spinal sources:
Spinal Causes of Neck Pain
- Degenerative disc disease and / or facet joint degeneration (discussed below)
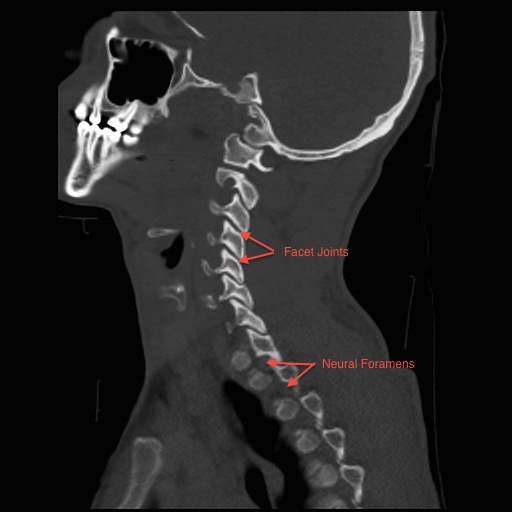
- Nerve compression due to a disc prolapse or stenosis (narrowing of the spinal canal or neural foramens) – this is described in the Arm Pain and Myelopathy section
- Cervical instability e.g. degenerative spondylolisthesis – this can occur in exactly the same way that it does in the lumbar spine – an example is in the Arm Pain and Myelopathy section
- Whiplash (discussed below)
- Torticollis (discussed below)
- Spinal Trauma, Infection and Tumours
- Inflammatory conditions such as Ankylosing Spondylitis and Rheumatoid Arthritis
Non-Spinal Causes of Neck Pain
- Stress
- Shoulder problems
- Brachial plexitis (problems with the nerves around the shoulder)
- Neuromuscular and neurological conditions such as dystonia
- Thoracic outlet syndrome
- Carotid artery problems
- Cardiac problems
- Head and neck infections and tumours
Degenerative Neck Pain – Degenerative Disc Disease and / or Facet Joint Degeneration
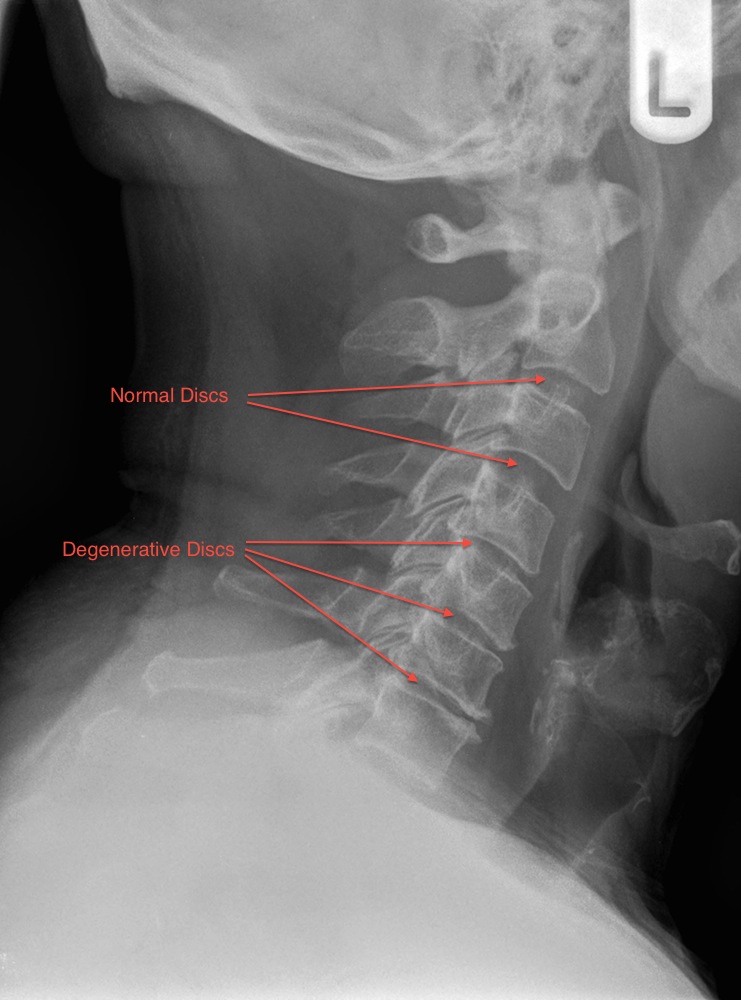
This is the normal ageing process and occurs in exactly the same way as described in the low back pain section. It is often termed Cervical Spondylosis. During the normal ageing process the intervertebral disc loses water and becomes stiffer. The disc can be thought of as a car tyre - over time it deflates and bulges. As this occurs the height is lost at the front of the spine and the facet joints at the back of the spine start to take more load. Facet joint wear then occurs. These processes can cause neck pain. However, a significant number of asymptomatic individuals will have degenerative changes on radiological imaging of their cervical spine and it does not cause them any problems. This is why it is termed the normal ageing process and it is predominantly genetic in origin. Patients with degenerative disc disease in the low back will often have it in the neck and vice versa (we term this tandem changes).
The natural history of this condition is favourable and up to 80% of neck pain sufferers show an improvement in their pain given the passage of time. However, chronic disabling symptoms can be present in up to 20% of patients. It can be very difficult to provide a surgical solution to patients with degenerative neck pain because there are over 20 joints in the cervical spine and many of these can show degenerative changes. Identifying the exact source of the pain can be challenging. Surgery for multilevel degenerative disease has unpredictable results and can cause more harm than good. Treatment usually involves non-operative measures such as medications, physiotherapy programmes, core stability exercises, Pilates, yoga, tai chi, aqua-aerobics, osteopathy, chiropractic treatment, acupuncture, reflexology, massage and other such activities. As with discogenic low back pain surgery can improve neck pain in up to 70% of patients if a focal cause can be identified.
More information can be found from www.patient.co.uk.



Torticollis
Torticollis means “twisted neck” and is often referred to as wryneck. It is a common cause of neck pain and stiffness and often occurs after sleeping or sitting in an unusual position, carrying heavy loads or poor posture. There is often no obvious cause. It is common to wake up with the pain having been completely asymptomatic when going to bed the previous night. It is thought to be due to a minor sprain or irritation of a muscle or ligament in the neck. There is often muscle spasm on one side of the neck that twists the neck to one side. Most cases of acute torticollis settle down over a couple of days. Keeping your neck moving, taking regular painkillers and maintaining good posture help. Very occasionally it can become chronic and other less common causes need to be excluded by a healthcare practitioner.
More information can be found from www.patient.co.uk.
Whiplash
Whiplash is a term that describes pain in the neck region after the specific mechanism of hyperflexion and hyperextension. This commonly occurs during motor vehicle collisions when the head will rapidly be thrown forwards and then backwards. It most commonly occurs in young adults aged between 20 and 40 years. Following a motor vehicle collision, up to one third of patients subsequently diagnosed with whiplash will develop neck pain immediately, up to two thirds within 12 hours and almost 90% within 24 hours. The diagnosis is mainly based on clinical history and examination. The symptoms of whiplash include neck pain and stiffness; headaches; pain in the shoulder or between the shoulder blades; low back pain or thoracic back pain; pain or numbness in the arm and/or hand; difficulty concentrating or remembering; and irritability, sleep disturbance and fatigue.
There is no diagnostic test for whiplash (i.e. X-Ray, CT, MRI, Ultrasound, Bone scan). These tests are used to rule out acute injuries such as a fracture (broken bone). There are many theories as to the cause and source of the pain in whiplash syndrome but there is no diagnostic or radiological test to confirm or refute these theories. Theories include small tears in the facet joint capsule, intervertebral disc, anterior spinal muscles, anterior spinal ligaments, interspinal ligaments or micro fractures (small breaks) in the vertebral body endplates or facet joints.
The Quebec Task Force on Whiplash-Associated Disorders performed a comprehensive systematic review in 1995 and concluded that whiplash is a self-limiting condition with a favourable prognosis for most patients. In 1998 a large study was performed on 2810 patients waiting for compensation following a whiplash type injury. In the group of patients with an isolated whiplash type injury, 25% were better within one week and most were better within 1 month of injury. Only 2% of patients had not recovered at 1 year following the injury. In the group of patients who had other associated injuries as well as the whiplash injury, 19% were better within 1 week, 30% within 1 month and 4% had not recovered at the 1-year mark.
Whiplash has been associated with psychological changes. Patients tend to have normal psychological profiles early after their injury and it is the pain that leads to psychological sequelae in most. Depressive symptoms tend to manifest after 6 weeks (excluding post traumatic stress disorder) and this is similar to patients who suffer from accidents in which they sustain multiple fractures (broken bones). Driving anxiety tends to improve in all cases of whiplash. However, it has been found that mood disorder at 1 year following a diagnosis of whiplash is twice that of the normal population.
The medical literature supports early active mobilization with patient education in the management of whiplash. In other words it is important to start normal activity or physiotherapy early. Evidence has shown that soft cervical collars are less effective than this. Patients taking non-steroidal anti-inflammatory drugs tend to have better movement 2 weeks following the injury. Unfortunately once whiplash pain becomes chronic, the treatments become relatively ineffective. There is no role for surgery in acute whiplash. If a surgically treatable injury is found, such as a fracture (broken neck), then the diagnosis of whiplash is incorrect.
There is no consensus in the medical literature as to how many patients go on to develop chronic symptoms. 90% of patients tend to be symptom free by 3 months. There are various prognostic indicators that are associated with poorer outcome following a whiplash injury. These include rapid onset of pain; more severe pain; acute hospital admission; radiation of pain to upper limb; headache; neurological deficit, stiffness, tenderness; premorbid psychiatric disease; responsibility for dependents; above average premorbid GP attendance (unrelated disorders); older age; female sex; lower educational achievement; part time employment; heavy manual labour; pre-existing neck and low back pain; and previous whiplash.
Whiplash is often associated with litigation and prolonged litigation tends to be associated with patients suffering from more severe pain. Unfortunately, litigation settlement is not associated with symptom improvement or return to employment. Financial gain does not result in the resolution of symptoms. Interestingly, quicker recovery is seen in countries that have no fault compensation (e.g. Canada), historically less litigation (e.g. Greece) and where there is no compensation for whiplash (e.g. Lithuania).
In summary, whiplash is a diagnosis of exclusion in which the pathology (disease or pain causing process) is unknown. It generally gets better but can cause significant disability. It needs to be identified and treated early to prevent long-term conversion to chronic pain.
More information on whiplash can be found at www.patient.co.uk and from the North American Spine Society.